Anatomy
Most people have four tiny parathyroid glands which typically lie behind each lobe of the thyroid gland in upper and lower positions (two on each side). Each parathyroid gland is about the size and colour of a lentil. Normal parathyroid glands cannot be felt or seen on imaging. Abnormal parathyroid glands may be a different colour, enlarged or firm to touch.
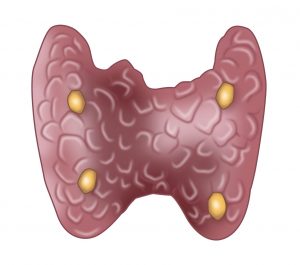
In 98% of people there are 4 parathyroid glands, which are located on the posterior surface of the thyroid gland in close relation to the recurrent laryngeal nerve.
Parathyroid Development
The parathyroid glands develop from the third and fourth pharyngeal pouches. The position of the glands reverses during adult life. The pair of parathyroid glands which is ultimately inferior develops from the third pouch with the thymus, whereas the pair of parathyroid glands which is ultimately superior develops from the fourth pouch. This explains the more varied location of the inferior parathyroid glans, with their longer path of migration.
Parathyroid Function
Parathyroid glands produce parathyroid hormone (PTH), which regulates the calcium levels in your blood. Hyperparathyroidism is essentially an overactive parathyroid gland and this leads to high levels of blood calcium. this can negatively affect your bone density, increase your risk of kidney stones and cardiovascular disease. About 1% of the population are affected by excessive parathyroid function.
Types of Parathyroid Disease
Parathyroid disease is almost always benign and can be classified by type:
- Primary (intrinsic problem within the parathyroid)
- Secondary (parathyroid functions abnormally in relation to another abnormally functioning organ eg. kidney)
- Tertiary (parathyroid continues to function abnormally even if the other abnormally functioning organ is fixed eg. after a kidney transplant)
In primary hyperparathyroidism one, two or all four parathyroid glands produce and secrete inappropriate amounts parathyroid hormone. This excess hormone results in high blood calcium levels which can cause numerous symptoms, some of which may go unnoticed. In most cases primary hyperparathyroidism is caused by a single abnormal gland, termed an adenoma. It is also possible to have two adenomas, called double adenomas. When all four glands are abnormal it is called ‘four gland hyperplasia’.
There are several recognised subtypes of primary hyperparathyroidism:
- Classic (high blood calcium, high parathyroid hormone)
- Normohormonal hyperparathyroidism (high blood calcium, inappropriately normal parathyroid hormone)
- Normocalcemic hyperparathyroidism (normal blood calcium, high parathyroid hormone)
Patients with parathyroid disease are commonly asymptomatic and have been diagnosed incidentally via blood tests done for another reason. Some patients have symptoms attributed to high blood calcium such as constipation, excessive thirst and urination, fatigue, recurrent kidney stones, anxiety and mental fogginess. Reduced bone density and fragility fractures are also associated with hyperparathyroidism. On balance, the symptoms which have been associated with primary hyperparathyroidism are extremely variable between patients, in nature and in severity.
About 10% of people with parathyroid disease have an underlying genetic condition.
Ultimately, the treatment of all types of parathyroid disease is parathyroid surgery.
Parathyroid Cancer
Parathyroid cancer is extremely rare and is often difficult to diagnose. Patients may have extremely high levels of blood calcium, a hard mass in the next or be completely asymptomatic. The treatment of parathyroid cancer is surgery.
The diagnosis of parathyroid disease is made with blood tests. A bone density or urine analysis may also be requested.
Parathyroid Localisation
The diagnosis of parathyroid disease is made with blood tests. A bone density or urine analysis may also be requested.
The aim of imaging in parathyroid disease, is to help localize the abnormal gland(s) in attempt to reduce the extent of dissection at surgery, NOT to confirm the diagnosis.
It is not uncommon to have imaging tests that are negative, but this does not mean that your diagnosis is wrong. Up to 30% of patients with parathyroid disease have imaging tests which are unyielding. Sometimes, even very abnormal parathyroid glands are not seen on ultrasound, nuclear medicine studies or CT scans but are still found at operation. Dr Edwina Moore will routinely perform a bedside ultrasound and request a nuclear medicine test called a SPECT/CT.
Treatment of Parathyroid disease
The only definitive treatment for parathyroid disease is surgery and in experienced hands the rate of cure is excellent (>98%). The aim of surgery is to safely remove all of the abnormal parathyroid tissue while leaving behind the normal parathyroid glands to maintain the body’s calcium balance. If some abnormal parathyroid tissue is left behind, you will not be cured. It may take several months after surgery for your blood tests to normalize.
Dr Edwina Moore uses several intra-operative techniques to ensure your best chance of cure. First, she repeats the ultrasound, once you are asleep. Not only does this allow a second look at the abnormal gland prior to starting, it helps to guide the most cosmetic incision. Other techniques are including frozen section and rapid parathyroid hormone assay. During her fellowship in the United States, she was also trained in the novel technique of parathyroid autofluorescence.

Dr Edwina Moore routinely performs a four-gland exploration, which means that during your operation she will inspect all of the parathyroid glands but will only remove the ones which are abnormal. The benefit of this technique is that it reduces the chance of leaving behind an abnormal gland (which would mean an unsuccessful surgery). Amongst endocrine surgeons, this is a highly controversial topic however Dr Edwina Moore strongly believes that it is a more thorough and logical approach.
After surgery you will be placed on a calcium replacement regime and at times Vitamin D. In most cases this is a temporary measure, until your remaining normal parathyroid glands regain function. Restoration of parathyroid function is determined by blood tests.
Parathyroid FAQs
- Is there any other treatment for hyperparathyroidism besides surgery?
No. Surgery is the only effective treatment of hyperparathyroidism.
- What will happen if I don’t have surgery?
Even if you think you have no symptoms, you will probably feel much better after you are cured. If you don’t have surgery, you will continue to have high blood calcium, and many symptoms. Without surgery, your bones will continue to become weaker, and possibly break. There is evidence of increased risk of high blood pressure, stroke, heart disease, and even shorter life expectancy, from untreated hyperparathyroidism.
- What are the risks of parathyroid surgery?
Potential risks associated with parathyroid surgery are:
- Permanent voice hoarseness
- Failure to cure the hyperparathyroidism
- Permanent hypoparathyroidis
- Infection of Incision
- Haematoma or Bleeding
- Seroma (fluid collection)
- Keloid or overgrown scar
- What is Familial Hypercalcemic Hypocalciuria (FHH)?
FHH is an extremely rare genetic condition that mimics patients with parathyroid disease. By contrast however, they often have a history of abnormal blood tests since childhood and other affected relatives. It is caused by an inactivating mutation in the CASR – patients have a high blood calcium and very low urine calcium. Surgery for these patients is not recommended and is non curative. The gold standard for the diagnosis of FHH is by genetic testing.
- Will I have a scar?
Yes. All incisions will heal with a scar. The aim is to perform a safe and appropriate operation, with the best cosmetic outcome (smallest, most discrete scar). Scars continue to remodel (and change in appearance) over 12months, up to 3 years. All patients heal (and therefore scar) differently. It is important to keep the wound clean, free from tension and covered from the sun. A thyroid scar is a horizontal scar on the neck. Dr EdwinaMoore will aim to place your scar is a natural skin crease so that is barely visible.
- When will I know the findings of the surgery?
Dr Edwina Moore will discuss the operation with you at multiple stages whilst you are in hospital. Blood tests on the first post-operative day will help determine The final pathology report which requires meticulous study of the surgical specimen usually takes one week and therefore will be available at the time of your post-operative review.
- Will I have stitches?
You will have some internal stitches in the muscle that your body will absorb naturally. Your skin will be expertly closed with medical glue and a steri-strip. There will be no skin stitches that need removal. This technique ensures an optimal cosmetic outcome.
- Will I have any physical restrictions after my surgery?
In general, your activity level depends on the amount of discomfort you experience. Most patients return to work in a week or two, and you are able to drive as soon as your head can be turned comfortably without discomfort. For the best wound healing it is advisable not to perform any heavy activity (eg. Lifting >7kg) for 4 weeks after surgery. It is also not advisable to bathe or swim with a fresh wound.
- What is the long-term follow-up?
For reasons that we don’t completely understand, some patients develop recurrent parathyroid disease often many years after successful surgery. This is different to a failed operation or persistent hyperparathyroidism. For this reason, Dr Edwina Moore will recommend annual follow-up after surgery with you following surgery. It is important not to miss recurrent disease as the manifestations of high calcium can negatively affect multiple physiological functions.